Open Green Spaces
The following visualisations were made using data collected from the London Datastore and can be found here.
Definitions
It is important to understand what constitutes as ‘open access’ as this allows us to clearly understand the data and could furthermore aid the analysis;
Meaning of Open Access Data: Public open space is designated according to ‘Access’ attribute information contained within GIGL open spaces dataset i.e. values such as ‘open, free’ are accepted as allowing access to public. Homes further away than the maximum recommended distance are considered to be deficient in access to that type of public open space.
In 2015 the recommended distances for each type were:
R – Regional Parks = 5km max
M – Metropolitan Parks = 2.4km max
D – District = 1.2km max
LSP – Local, Small and Pocket parks = 400 metres max
https://uclqcde.carto.com/builder/c05eb6bc-cbc8-11e6-a73f-0e05a8b3e3d7/embed
Note if legend does not appear on the map, please enlarge screen.
Figure 4.1 – London choropleth map illustrating percentage of population with access to green spaces in 2013 per Borough.
Choropleth map analysis
In this map the darker areas depict the boroughs with greater percentage of access to green spaces, while the lighter areas consequently depict those with lower access to green spaces. On average, 41.2 of the population has access to open spaces (according to the data illustrated in figure 4.1), however the data varies greatly between boroughs, with boroughs such as Hackney illustrating a high percentage of access to open spaces (67.8%), and boroughs such as Hillingdon depicting low access to open spaces (29.4%). Hackney (67.7%), Tower Hamlets (58.5%) and Haringey (57%), seem to have the greatest population with access to open space, results that are slightly surprising given the lack of major green spaces (compared to for example Richmond Upon Thames) in its proximities. After looking in greater depth it becomes evident that these do have a wide range of smaller public parks available to the public that are located across the borough, which would enhance the overall chance of having access to one. Similarly, they contain a variety of other ‘open spaces,’ (specified below), explaining why its numbers are notably higher.
Boroughs such as Hillingdon show low access to open spaces, which is initially surprising given the major amounts of green space (due to Colne Valley Regional Park) evident within its premises. These green spaces, however, are not entirely freely accessibly to the public (since many are reservoirs and parks, often requiring payment for entrance, or undergoing closure at sundown) and given the data only includes free, easily accessible spaces, it explains why they are not included in the data. Furthermore, parts of the evidently open spaces are located around Heathrow, which would furthermore not be accessible to the public, and thus are disregarded in the data for open spaces.
Comparing the obesity map with figure 4.1, we can deduce a correlation between access to open and green spaces and percentage of obesity per borough. For a relationship between obesity and open spaces to occur we would expect the darkest area (Blue) in the obesity map (hence highest percentage of obesity) to correlate with the lightest area (faint green) of the open spaces map (hence lowest access to open spaces). Most of the darker boroughs in figure 4.1 are indeed much lighter on the scale of the obesity map. It is evident from the map that the higher prevalence of obesity boroughs including (but not limited to) Hillingdon (21.9%), Croydon (22.7%), and Havering (24.8%) show a lower percentage of access to open and green spaces ranging between a meagre 27 to 30%.

Figure 4.2 – Scatter plot illustrating the correlation between the percentage of population obese and the percentage of population with access to open space per Borough.
Spearman’s Rank Correlation Coefficient: -0.393 (3 s.f.)
Scatter plot analysis
From the scatter plot above, the correlation coefficient for this factor is weak to moderate (-0.393). The line graph suggests a faint negative correlation (looking at the line of best fit); the greater the percentage of households with access to open space, the lower the prevalence of obesity. Indeed, many studies in the past have suggested a link between between better health outcomes (including lower prevalence of obesity) and greater access to green space, given the apparent increase in levels of physical activity by individuals living in ‘greener’ areas. According to a study by Mytton et al. a positive association between green space and overall physical activity is evident. The “odds of achieving recommended physical activity” when having greater access to green space were significantly higher in urban areas (Mytton, 2013). Open spaces are usually well equipped with “recreational amenities” such as cycling and walking, and hence the correlation with physical exercise is no surprise (Ghimire, 2015). Open spaces therefore indirectly correlate to a reduction in obesity, given the increased incentive to do exercise. Notably, these positive correlations are often weak, similar to the correlation data demonstrated in figure 4.2. Hence, amounts of uncertainty remain regarding the overall correlation, and further research needs to be done.
Limitations of Data
This measure takes no account of the quality or facilities at each open space. Hence, while a particular space might be accessible to the public, it does not mean they are perfect when it comes to exercising or moving around significantly. For example, some open spaces are of historic value, such as churchyards, which are evidently not ideal for exercising. Hence ‘open data,’ while it includes green parks ideal for exercising and movement, does not necessarily signify spaces perfect for exercise.
Sports Facilities
The following visualisations were made using data collected from the London Datastore and can be found here.
https://uclqcde.carto.com/builder/0e768b80-c39b-11e6-b254-0e3a376473ab/embed
Note if legend does not appear on the map, please enlarge screen.
Figure 3.3 – London choropleth map illustrating number of sports and leisure facilities per 1000 people per Borough.
Choropleth map analysis
The Sports Facilities map displays the number of sports and leisure facilities per 1000 people per Borough, and was created in order to find links between high obesity areas and the population’s access to exercise facilities. We had initially assumed that areas with more facilities available to the public would correspond with areas with the least prevalence of obesity, as we also assumed that people tend to use the facilities in proximity to their homes.
The map shows that the average number of sports facilities per 1000 people is 2.37. However, when looking at the map it is important to note that it may seem slightly misleading, as the highest number of facilities is 15.7 per 1000 people, meaning that for the darkest colours, the numbers vary hugely. For instance, Both Kingston upon Thames and City of London appear in the darkest shade, but Kingston upon Thames only has 2.4 facilities per 1000 people, whereas City of London has 15.7.
When looking for trends between this map and the Obesity one (link), there is no significant pattern to be seen. In fact, areas where we assumed there would be more facilities due to their lower obesity rates, (Richmond upon Thames, Wandsworth, Lambeth, Tower Hamlets, Camden, Kensington and Chelsea) tend to also be areas with very few facilities, with the exception of Richmond upon Thames.

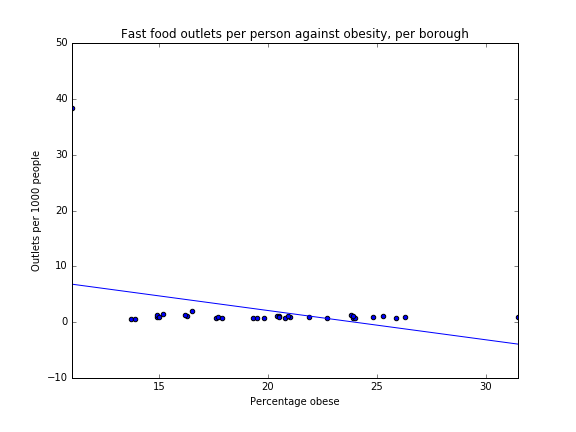
Figure 3.4 – Scatter Plot illustrating the correlation between percentage of obesity and number of sports facilities per 1000 people of the population.
Spearman’s Rank Correlation Coefficient: -0.0246 (3 s.f.)
Scatter plot analysis
A Spearman’s Rank Correlation Coefficient was calculated and shows an incredibly weak correlation of -0.0246 (3 s.f.). This shows that there is no real trend to be found between areas in which facilities exist and areas with the most prevalence of obesity. Accordingly, the scatter plot comparing these two factors also shows that there is no clear pattern, with the majority of boroughs containing between 1-3 facilities per 1000 people. City of London and Ealing are exceptions to this, with 15.7 and 13.9 facilities per 1000 people respectively. Apart from this huge increase, the number of facilities per borough would have stayed very similar (around 2 per 1000 people), which could point to other factors, not a lack of facilities, leading to less sports participation and increased obesity rates.
The reasons behind a lack of correlation between obesity and the prevalence of sports facilities could be a variety of things. First, people may use gym or sports facilities closer to their areas of work, rather than in the boroughs they reside in. Also, sports and leisure facilities can take up a significant amount of space, depending on what type of activities they were created for. Therefore, the creation of sports facilities may be linked more strongly to availability of space, or cost of construction, than to actual demand. Also, the data did not reveal whether or not the facilities were open to the public and free or if they included fees. This would therefore have a link with income, and further limit people’s ability to use such facilities.
Since there was no clear correlation between facilities and obesity, it is hard to come to any conclusions on how the government could better fund these areas. Therefore, we chose to create a Sports participation map (see below), to show which boroughs were the most active in London, and with the hopes of better identifying areas which need further encouragement and help from the government to partake in physical activity.
Limitations of Sports Facilities Data
There was a lack of distinction between sports facilities run by the government, that consequently received government budgets, and privately run businesses.
Moreover, the data does not distinguish between facilities that belong to schools or colleges, which are unlikely to be open to the public. Thus, while these are counted in the data set, they are not actually available to the whole population, and not of value in this context.
Furthermore, it was difficult to distinguish which school and colleges had a range of facilities and which had little, thus it does not represent the quality of the various facilities.
Finally, the data does not mention costs of facilities and memberships per facility, which would have provided us with interesting information regarding the affordability of facilities across London, and in turn offer insight on the accessibility of facilities in economic terms.
Sports Participation
The following visualisations were made using data collected from the London Datastore and can be found here.
https://uclqcde.carto.com/builder/6907c78a-cd0a-11e6-9a93-0ecd1babdde5/embed
Note if legend does not appear on the map, please enlarge screen.
Figure 3.5 – London choropleth map illustrating percentage of population participating in sports 3 times a week.
Choropleth map analysis
The Sport Participation choropleth map displays the percent of a population per borough that participate in physical activity three times a week in 2014 and 2015. This map was created in order to show a clearer link between the lifestyle choice of partaking in physical activity and its relationship to obesity, as well as to compliment theories surrounding factors such as income and education levels. It was also created due to the issues arising from the “Sports facilities” map, which we found to not represent physical activity trends of the people living in boroughs.
According to the NHS’ official recommendations on the treatment of obesity, “maintaining a healthy weight requires physical activity to burn energy”(National Health Service). Therefore, when creating this map we were hoping to find that the areas with the highest prevalence of obesity would be the ones with the least recorded percentage of sports participation.
For the most part, our prediction is correct. Areas with the percentage of most participation are darkest in shade and range from 28.2% to 24%(Richmond upon Thames, Wandsworth, Merton, Kensington and Chelsea, Hammersmith and Fulham), followed by slightly lower percentages from 22.8% to 20.8% (Haringey, Islington, Camden, Westminster, Lambeth and Bromley). Areas with the least prevalence in obesity are shown in the lighter colours, and there is a significant overlap in areas such as Wandsworth, Richmond upon Thames, Lambeth, Kensington and Chelsea, Camden, Haringey, Islington, Hammersmith and Fulham and Westminster.
When comparing this map to that of Income per borough, one can see that areas with less income tend to also participate in less physical activity. This is not surprising, as a study has found that income and physical activity are linked; with “each additional ten thousand dollars in income increases the probability that an individual participates in some physical activity by 1 percent” (Humphreys and Ruseski, 2006). This could be linked to the cost of partaking in physical activity- nowadays many people use various facilities, such as gyms, swimming pools, personal fitness machines. All of these, as well as exercise equipment and clothes, cost money, and therefore people with higher incomes are probably more willing to spend money, and thus spend more time participating in physical activity (Humphreys and Ruseski, 2006).
Similarly, when compared to the educational map, one can see that areas with higher percentages of degree attainment also participate in more sports. This could reflect how sports education in schools are important and effective in determining people’s lifestyle choices after their education years, and how further funding into lifestyle and sports education at schools could increase the chances of better choices for more people. In addition, higher degree attainment has a link with income as well.
When comparing the map to the percentage of Fast Food outlets map, there is no clear pattern to be seen, although one would have originally assumed that people who do more sport would also have better eating habits. However, the fast food map does not reflect the eating habits of the population, and instead reflect the demand for well-known outlets in popular places, the city center or in places of work.

Figure 3.6 – Scatter Plot illustrating the correlation between percentage of obesity and percentage of sports participation.
Spearman’s Rank Correlation Coefficient (SRCC): -0.794 (3 s.f.)
Scatter plot analysis
This information above is further supported by a strong negative correlation (-0.79) on the Spearman’s Rank Correlation Coefficient, which shows that areas whose population have the highest rates of participating in physical activity 3 times a week also show the lowest rates of obesity, and therefore suggests a strong link between the two factors. Additionally, we created a scatterplot showing ‘Sports participation against obesity, per borough’. This is another visual representation which shows a strong correlation between the two. Although these results are highly correlated, there are, of course, many factors other than physical activity levels that contribute to obesity. However, given that the average percent of the population to participate in physical activity 3 times a week is only 18.7%, there is definitely room for the government to further encourage sports participation in the general public.
Limitations of Sports Participation Data
The limitation with this data is that it only shows the percentage of people who participate in physical activity three times a week. It does not include data for people who participate in physical activity more or less than that, which could have given a clearer view on which boroughs participate in the most physical activity in general. Additionally, while it specifies “three times a week”, it does not specify the time of each session nor the intensity, which could also affect the overall results in showing the most active boroughs.
Also, the dataset does not specify how the data was checked, and therefore the results are what the population has self-reported. In accordance, this could mean that certain people may be untruthful about their levels of physical activity, which would make the results less reliable.
Lastly, there was no data available for City of London borough, which will have slightly affected the Spearman’s Rank Correlation Coefficient and could have shown either a stronger or weaker result.
References
Ghimire, R., Green, G., Ferreira, S., Poudyal, N. and Cordell, H. (2015). Green Space and Adult Obesity Prevalence in the United States. [online] Available at: http://ageconsearch.umn.edu/bitstream/196812/2/green%20space%20obesity.pdf.
Humphreys, B. and Ruseski, J. (2006). Economic Determinants of Participation in Physical Activity and Sport. 1st ed. International Association of Sports Economists, pp.2-19.
Mytton, O., Townsend, N., Rutter, H. and Foster, C. (2012). Green space and physical activity: An observational study using Health Survey for England data. Health & Place, [online] 18(5), pp.1034-1041. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3444752/.
National Health Service. (2016). Obesity – Treatment – NHS Choices. [online] Available at: http://www.nhs.uk/Conditions/Obesity/Pages/Treatment.aspx [Accessed 16 Jan. 2017].